NH company shines light on UV therapy for autoimmune conditions
Started in 2021, Cytokind describes itself as 'the global leader in using UVB light to treat immune disorders and improve survival and the quality of life for patients'
 New Hampshire residents pay the lowest amount for health insurance when compared to income in the nation, according to a new study. Enjoy it while you can. Changes in state and federal law will likely increase premiums in the Granite State in the coming years.
New Hampshire residents pay the lowest amount for health insurance when compared to income in the nation, according to a new study. Enjoy it while you can. Changes in state and federal law will likely increase premiums in the Granite State in the coming years.
The state ranked 50th in a study that compared average silver plan, or benchmark, insurance premiums to median income in every state. New Hampshire residents with a silver plan use 4.02% of their income to pay for health insurance, according to the WalletHub study.
The percentage is an estimate, based on premiums for silver tier insurance plans published by the Kaiser Family Foundation, a nonprofit that analyzes health care costs. Silver plans have a moderate deductible and fairly low premiums, and are considered the benchmark for insurance analysis. They’re available to people who use private insurance as well as those insured by Medicare and Medicaid. (Nearly as many New Hampshire residents enrolled in Affordable Care Plan insurance have a bronze plan as a sliver one, according to the Centers for Medicare and Medicaid, which is a higher payment tier.)
New Hampshire’s rank as 50 in the WalletHub study is also helped by the fact that the state has the highest individual median income of any state in the U.S., $87,356, according to the latest federal Census figures, just behind Washington D.C., at $88,190. Median means that half earn more, and half less.
Residents of neighboring Vermont, according to the study, use the highest percentage of their income for health insurance: 19.61%. Vermont’s median income is $76,949 and the average benchmark premium is $1,277, the highest in the nation.
The difference between the cost of premiums in the two states has a lot to do with access — in simple terms, Vermont has fewer large health care systems as well as fewer insurance options than New Hampshire does.
New Hampshire health insurance snapshot
An estimated 95% of New Hampshire residents have health insurance, including a record 70,337 enrolled in 2025 in the Affordable Care Act Marketplace, which provides lower-cost health insurance to people who don’t get it through an employer and is still sometimes referred to as “Obamacare.”
Though the number with ACA coverage represents a fraction of New Hampshire’s insured residents, premiums, before subsidies, are similar to what’s offered under private insurance.
About 60.2% of the state’s residents have private health insurance, most through an employer, according to the New Hampshire Fiscal Policy Institute. Another 17.4% have public insurance, including Medicare, Medicaid and VA coverage.
Some of the reasons health insurance premiums are low in New Hampshire are:
The number of uninsured residents in the state has dropped from 10.7% in 2013 to 4.5% in 2025. In the past four years, record numbers of residents have enrolled in ACA, largely because of increased subsidies for the program through the American Rescue Plan, which were extended through 2025 through the Inflation Reduction Act. The federal subsidies come in the form of an Advanced Premium Tax Credit (APTC), which is technically how ACA insurance premiums for moderate and low-income users are reduced so that they don’t pay the full premium price.
Medicaid expansion in the state led to the Granite Advantage Program, created in 2019, which allows people between 19 and 64 with incomes up to 138% of the federal poverty level to get lower-cost coverage. In 2025, that’s a gross income of $21,597 for an individual, $29,187 for a family of two, $36,777 for a family of three, and so on.
New Hampshire in 2023 created a reinsurance program that reduces financial risk for insurance companies, which means they can offer lower premiums to customers. It’s similar to one that Maine established in 2011.
The state’s ACA Marketplace has five insurance providers, which makes it more competitive than states that have less of a free-market approach.
New Hampshire health insurance outlook
While the reinsurance program and free-market approach will help keep New Hampshire residents’ premiums lower than what will be coming in some other states, the state won’t be immune.
The budget bill signed by the President July 4 as well as New Hampshire’s FY 2025-26 budget, signed into law by Gov. Kelly Ayotte on June 27, will spur an increase in health insurance premiums over the coming years.
While the new state and federal policies affecting what people will pay for health insurance don’t apply to employment-based private insurance, there’s a ripple effect when that will eventually cause everyone’s health insurance costs to rise.
When the low- and moderate-income New Hampshire residents affected by the federal and state changes can’t afford health insurance, delay health care, or get knocked off of their programs for bureaucratic reasons, people don’t stop getting sick or needing medical care. Someone has to pay for it, so health care costs for everyone go up, which means insurance costs do, too.
Many of the impacts will take a couple years to show, especially some of the federal provisions that don’t go into effect until the end of 2026.
New policies on both the state and federal level that will likely result in a rise in insurance premiums in New Hampshire are:
New Hampshire residents in the Granite Advantage Health Care Program will have to pay monthly premiums ranging from $60-$100, depending on family size, beginning in July 2026 under the new state budget.
Premiums will increase for those in New Hampshire’s Medicaid-funded Children’s Health Insurance Program (CHIP), which provides health insurance for children in families that otherwise couldn’t afford it, to $190 for a family of two, $230 for a family of three, and $270 for family of four or more under the new state budget.
Medicaid recipients will be required to pay $4 “cost-sharing” for prescriptions under the new state budget.
Unless state law is changed, the Granite State Advantage program will be eliminated if the federal Medicaid expansion contribution drops below the current 90%. The amount provided to the 40 states that opted for Medicaid expansion is reduced in some circumstances, though it’s not clear yet what the impact will be.
Enhanced ACA tax credits under the Biden administration expire at the end of the year, and were left out of the federal law, meaning higher premiums for all ACA enrollees.
Those who make more than 138% of the federal poverty guideline and have ACA insurance will have to pay out-of-pocket copays of $35 or more for services and procedures that previously didn’t have a copay. They will also pay increased prescription drug costs.
Abortion and some other reproductive services for women will no longer be covered by ACA insurance, not only removing vital health care for women, but leading to higher-cost conditions that aren’t treated, as well as the high cost of giving birth to and raising children. (There are no restrictions regarding coverage for vasectomies and male reproductive procedures.)
Most Medicaid expansion ACA recipients (including those in Granite State Advantage), will have to meet work requirements that will have to be documented regularly. According to KFF, most people affected already work, but the new rule will likely knock people off the program who miss documentation deadlines or can’t navigate the paperwork. In Arkansas, which implemented work requirements, more than 18,000 people lost coverage, many because they didn’t report or reported incorrectly. Studies have also shown that more requirements lead to more administrative errors and slowdowns that have a negative impact on recipients.
Automatic re-enrollment ends, meaning those with ACA will have to fill out an enrollment form every year, and the open enrollment period to do it has been reduced to Nov. 1-Dec. 15, rather than the current Nov. 1-Jan. 15. Industry experts say this means fewer people will enroll because they’ll miss the deadline, not realize they need to re-enroll, or have difficulty with the paperwork. It also causes more administrative duties and paperwork, which will lead to errors and slowdowns at understaffed state and federal offices.
Year-round special enrollment for people who make 150% or less of the federal poverty guideline is eliminated. Those who lose their insurance, for instance through a job loss or divorce, will have longer wait times for ACA, particularly if they are getting a subsidy. It may take 90 days or more to get coverage.
Beginning in 2027, states will have to conduct checks on Medicaid enrollees every six months, including verifying income, place of residents, and more. This will lead to a lot of red tape and delays, which will knock people off the program or delay their benefits.
This article is being shared by partners in the Granite State News Collaborative. For more information, visit www.collaborativenh.org.

Started in 2021, Cytokind describes itself as 'the global leader in using UVB light to treat immune disorders and improve survival and the quality of life for patients'

Lebanon company’s technology helps surgeons pinpoint size, shape of tumors

Amid statewide shortage, schools and hospitals aim to increase workforce
Some state officials and lawmakers are concerned that New Hampshire’s incoming Medicaid premium system may conflict with provisions in Congress’ One Big Beautiful Bill Act.
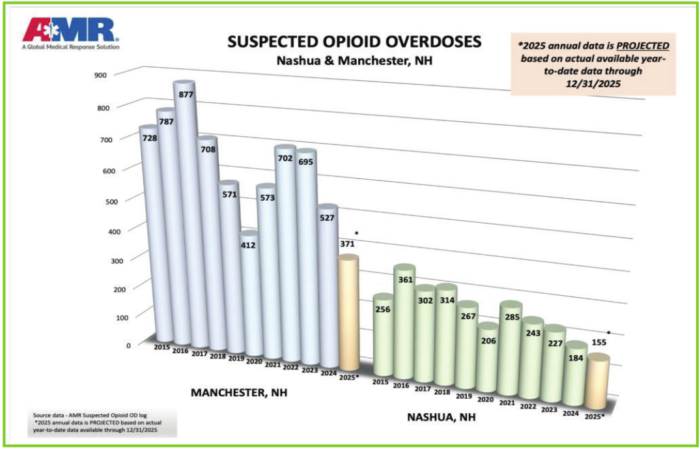
American Medical Response (AMR) released its annual suspected opioid overdose statistical report earlier this month for New Hampshire’s two largest cities, Manchester and Nashua. Both communities experienced record low numbers.

Providing benefits aimed at meeting diverse needs may provide a more affordable approach to care
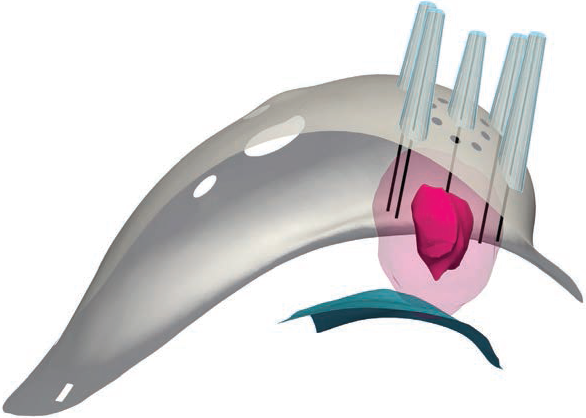
Cairn Surgical, Inc., a medical technology firm based in Lebanon, NH, announced earlier this month that patient enrollment has been completed in the U.S. pivotal trial of its Breast Cancer Locator (BCLTM) System.

Now that 2026 is underway, New Hampshire employers should turn their attention to the state’s new Parental Medical Leave law (PML). Effective January 1, 2026, most employers with 20 or more employees are required to provide unpaid leave to allow employees to attend childbirth-related medical appointments, postpartum care and pediatric visits during a child’s first year.

The federal government will give with one hand and take with another when it comes to New Hampshire’s rural health care system in 2026.






